Look Beyond the Symptoms: A Systems Lens for Creating Operational Excellence in ABA Organizations
The setup
The previous article in this newsletter argued that hiring decisions are culture decisions, and that values alignment between clinicians and the organizations that employ them is a retention variable the field has often treated as a soft preference. Values alignment is one variable. The peer-reviewed literature on behavior technician and BCBA retention names many others, including supervisor support, satisfaction with training, satisfaction with pay, role clarity, and working conditions (Kazemi et al., 2015; Nastasi et al., 2024; Novack & Dixon, 2019). Many of the retention, fidelity, growth, and access problems observed in ABA practice organizations are structural in nature.
When a practice owner faces one of these structural problems, the next decision is what to do about it. The response often defaults to the same pattern: a new training, a new feedback protocol, a new performance review, a new incentive. The intervention is aimed at the level where the problem appeared. The performer is trained, the symptom improves for a period, and the same problem reappears in the next person hired to do that job. This article gives you a procedure for reading the problem before designing the intervention so that the work you do at the level you choose has a chance of holding.
Why most ABA interventions do not hold at the organizational level
Behavioral systems analysis (BSA) is the application of behavior analysis to organizations conceptualized as integrated systems of interlocking behavioral contingencies and organizational processes (McGee & Diener, 2010; McGee & Crowley-Koch, 2019). Drawing from systems theory, performance systems analysis, and organizational behavior management, BSA examines organizational performance across multiple levels of analysis, including the organization, the process, and the performer (Rummler & Brache, 2013; Malott, 2003; Addison et al., 2009).
The organization level addresses strategic direction, structure, accountability, and the alignment of stated goals with the measures and feedback systems used to track them. Mission, values, organizational design, and external feedback are organization-level constructs. The process level addresses workflow, specifically how inputs are converted into outputs and how work moves from one function to another. In ABA practice organizations, this is the level at which authorizations, intake, scheduling, clinical documentation, supervision cycles, and billing operate. The performer level addresses the individual worker, the antecedents, behaviors, and consequences experienced by the people doing the work.
The three levels are arranged in a causal hierarchy. Organization-level conditions produce process-level outcomes, which produce performer-level results. The level at which a problem originates determines the level at which intervention has to occur, and performer-level interventions are unlikely to produce durable resolution when the origin of the problem is organizational.
Gravina, Villacorta, Albert, Clark, Curry, and Wilder (2018) reviewed organizational behavior management research in human service settings from 1990 to 2016 and found that of the 75 articles meeting inclusion criteria, the overwhelming majority targeted the performer level. Wilder, Lipschultz, King, Driscoll, and Sigurdsson (2018) reported that even at the performer level, pre-intervention assessment was conducted in a minority of published studies. The science is sound; however, much of the literature has focused on performer-level intervention, despite many organizational problems involving variables operating at the organizational and process levels.

A reading procedure
The procedure has five steps. It takes about thirty minutes to run on a given problem, and it produces a defensible answer to one question: at what level should the intervention be designed?
Step 1. Name the symptom.
Write the problem in a single sentence that names a specific behavior, the person performing it (or failing to), and how often it occurs. "RBT morale is low" is not a symptom statement. "Two of our six RBTs in the West clinic have missed at least three scheduled sessions in the past four weeks without re-scheduling" is. The discipline of specificity at this step prevents the analysis from running on an abstraction. If the symptom cannot be named at this level of specificity, the problem has not been observed clearly enough to act on, and the next step is observation rather than intervention.
Step 2. Test for regeneration.
Ask whether the same problem has appeared before in a different person, or in the same person after a previous intervention. Missed sessions in two RBTs is a different diagnosis than missed sessions across eight RBTs over the past year. The first may be performer-level. The second is more likely to involve structural variables. The test for regeneration is the most useful single move in this procedure, because it separates problems that respond to performer-level intervention from problems that will not. A regenerating problem is a signal that the conditions producing it sit upstream of the person who is currently expressing it.
Step 3. Trace the process.
Identify the workflow that produces this work being done this way. In an ABA practice this means tracing the supervision cadence, the scheduling system, the documentation requirements, the handoffs between scheduling and clinical, the feedback the technician receives, and the consequences attached to performance. The question is whether the process holds the technician to the standard or whether the process permits the standard to drift. Kazemi, Shapiro, and Kavner (2015) found that satisfaction with supervision and satisfaction with initial training were among the strongest predictors of behavior technician turnover intent. Gibson, Grey, and Hastings (2009) found that perceived supervisor support predicted burnout among therapists in ABA schools. Both findings are consistent with process-level variables influencing retention and burnout. The process level is often where regenerating performance problems first become visible to a careful reader
Step 4. Trace the organization.
Ask what conditions allow the process you just described to continue producing this outcome. Standards, accountability, measurement, and leadership cadence are the relevant categories. If the supervision cadence in Step 3 is monthly rather than weekly, the organization-level question is who decided the cadence, whether anyone is reviewing whether it produces the clinical outcomes the practice has committed to, and what would have to happen for that cadence to change. The organization-level analysis is rarely glamorous. It is usually a matter of identifying a standard that exists in writing but is not measured, a measure that exists but is not reviewed, or a review that occurs but produces no consequence. Nastasi and colleagues (2024) found that RBTs frequently described structural conditions, including inconsistent training, scheduling, and access to supervision, as drivers of burnout and turnover. These findings suggest organization-level conditions that may contribute to process-level dysfunction and downstream performer turnover.
Step 5. Design at the level of origin.
The level at which the analysis identified the origin is the level at which the intervention is designed. If the analysis implicates the organization level, the work begins there and sequences downward. Organization-level work without process-level follow-through stalls. Process-level work without organization-level support reverts. Performer-level work without process-level reinforcement does not generalize. The order matters. The discipline this step requires is that the intervention does not default back to the performer level because performer-level work is faster to launch and easier to measure in the short term.
A worked example
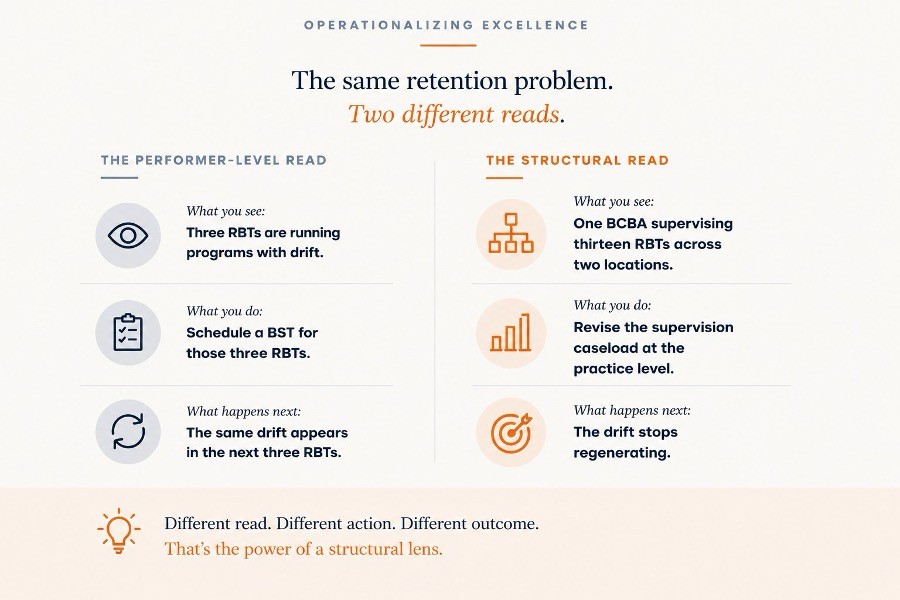
A practice owner notices that treatment fidelity has dropped in the West clinic. Three RBTs are not running programs as written. The owner is preparing to schedule a behavioral skills training (BST) session for those three RBTs.
Step 1: The symptom is three RBTs in one clinic implementing programs with measurable drift on specific protocols, over the past six weeks.
Step 2: This has happened before. Two RBTs left the West clinic in the prior quarter citing inconsistent supervision. The problem is regenerating.
Step 3: The BCBA assigned to the West clinic is supervising thirteen RBTs across two locations and has been able to observe each RBT directly approximately once every three weeks. The supervision cadence may be permitting drift because it is not catching deviation early enough to correct it.
Step 4: The supervision caseload was set at the practice level eighteen months ago when the organization had fewer RBTs and one location. No one has revised it. There is no measure of supervision frequency in the monthly clinical leadership review.
Step 5: The BST alone is unlikely to resolve the problem. The intervention is to revise the supervision caseload standard at the practice level, restructure the West clinic’s supervision allocation, and add supervision frequency to the monthly clinical leadership review. The BST may still be useful, but it sits downstream of the structural work and is sequenced after it.
What is next in the series
This article opens a sequence of pieces in Operationalizing Excellence drawn from Building Organizational Excellence: A Behavioral Systems Approach for ABA Practice Owners. The white paper specifies eleven behavioral domains of organizational health across three BSA levels and four developmental stages of organizational maturity. Each domain becomes generative material for diagnostic and operational articles in this newsletter.
The next article in the series examines the founder oversight ceiling, the structural condition that caps ABA practice organizations at the size of the founder’s personal capacity. The piece traces the founder oversight pattern through the same three-level lens introduced here and identifies the organization-level and process-level conditions that allow a practice to grow past it.
References
Addison, R. M., Haig, C., & Kearny, L. (2009). Performance architecture: The art and science of improving organizations. Pfeiffer.
Carr, J. E., Wilder, D. A., Majdalany, L., Mathisen, D., & Strain, L. A. (2013). An assessment-based solution to a human-service employee performance problem: An initial evaluation of the Performance Diagnostic Checklist—Human Services. Behavior Analysis in Practice, 6(1), 16–32. https://doi.org/10.1007/BF03391789
Gibson, J. A., Grey, I. M., & Hastings, R. P. (2009). Supervisor support as a predictor of burnout and therapeutic self-efficacy in therapists working in ABA schools. Journal of Autism and Developmental Disorders, 39(7), 1024–1030. https://doi.org/10.1007/s10803-009-0709-4
Gravina, N., Villacorta, J., Albert, K., Clark, R., Curry, S., & Wilder, D. A. (2018). A literature review of organizational behavior management interventions in human service settings from 1990 to 2016. Journal of Organizational Behavior Management, 38(2–3), 191–224. https://doi.org/10.1080/01608061.2018.1454872
Kazemi, E., Shapiro, M., & Kavner, A. (2015). Predictors of intention to turnover in behavior technicians working with individuals with autism spectrum disorder. Research in Autism Spectrum Disorders, 17, 106–115. https://doi.org/10.1016/j.rasd.2015.06.012
Malott, M. E. (2003). Paradox of organizational change: Engineering organizations with behavioral systems analysis. Context Press.
McGee, H. M., & Crowley-Koch, B. J. (2019). Using behavioral systems analysis to improve large scale change initiatives in autism service organizations. Perspectives on Behavior Science, 42(4), 931–954. https://doi.org/10.1007/s40614-019-00231-0
McGee, H. M., & Diener, L. H. (2010). Behavioral systems analysis in health and human services. Behavior Modification, 34(5), 415–442. https://doi.org/10.1177/0145445510383527
Nastasi, J. A., McGarry, K. M., Peters, K. P., Leon, Y., Bacotti, J. K., & Gravina, N. (2024). A qualitative analysis of variables contributing to Registered Behavior Technicians’ burnout and turnover in Florida. Behavior Analysis in Practice, 18(4), 1139–1151. https://doi.org/10.1007/s40617-024-01033-w
Novack, M. N., & Dixon, D. R. (2019). Predictors of burnout, job satisfaction, and turnover in behavior technicians working with individuals with autism spectrum disorder. Review Journal of Autism and Developmental Disorders, 6(4), 413–421. https://doi.org/10.1007/s40489-019-00171-0
Rummler, G. A., & Brache, A. P. (2013). Improving performance: How to manage the white space on the organization chart (3rd ed.). Jossey-Bass.
Wilder, D. A., Lipschultz, J. L., King, A., Driscoll, S., & Sigurdsson, S. (2018). An analysis of the commonality and type of preintervention assessment procedures in the Journal of Organizational Behavior Management (2000–2015). Journal of Organizational Behavior Management, 38(1), 5–17. https://doi.org/10.1080/01608061.2017.1325822
