When the ABA Practice Founder IS the System
The practice that runs on one person
I spent the early years of building an ABA practice convinced that the cracks I kept patching were a sign I needed to be more disciplined, more present, more involved. They were not. They were the predictable result of an organization that had no system beneath the founder, and I was the system. That distinction took me too long to see, and it is the distinction this article is about.
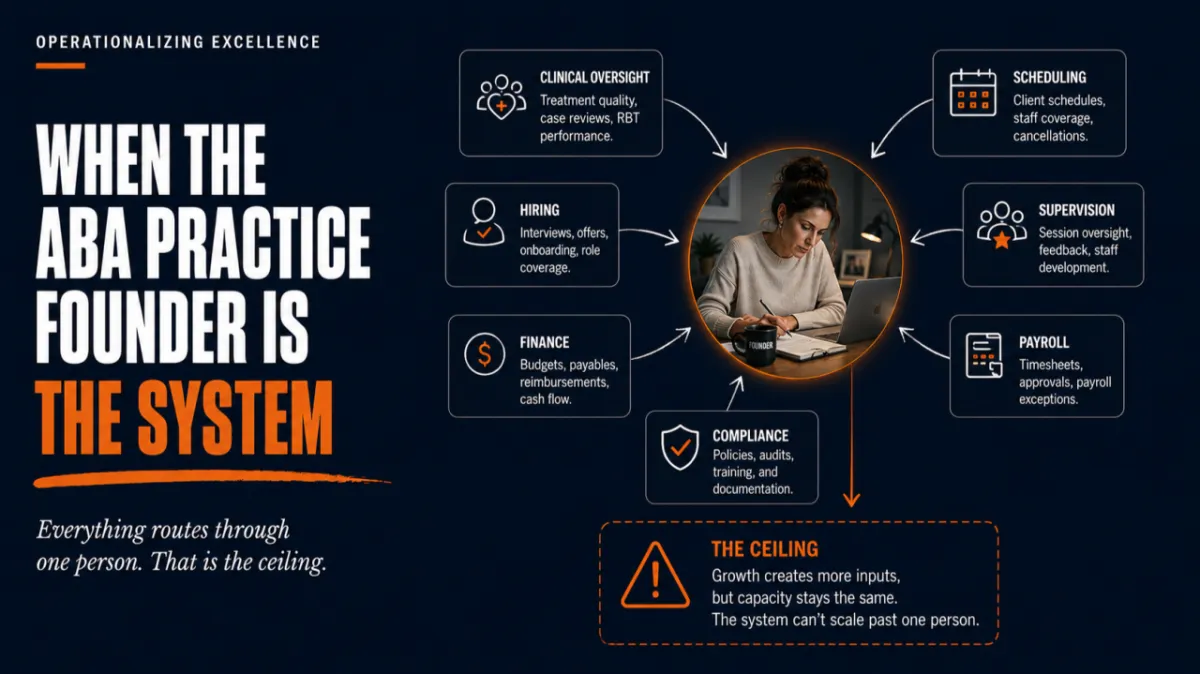
Most ABA practices are built by a clinician. A BCBA takes on a few clients, the caseload grows, the clinician hires technicians, and at some point the thing that started as clinical work becomes an organization. That founder is usually still the person who interviews every hire, reviews the hard cases, signs off on the schedule, watches the cash, and sets the standard for what good work looks like. The practice holds together because the founder holds it together. For a while, that works well enough that no one questions it.
The founder oversight ceiling is the point where it stops working, and the reason it stops has nothing to do with how hard the founder is willing to work. It is a structural condition. When the only mechanism delivering organizational standards to the front line is the founder’s personal attention, the organization can only grow to the size of what one person can personally observe. That size is reached well before the practice runs out of families who need services. The practice does not stall because demand dried up. It stalls because the founder ran out of capacity, and capacity was the system.
Why this looks like success right up until it doesn’t
The founder oversight ceiling is hard to see early because, in the beginning, founder oversight is genuinely excellent. The founder knows every client, every clinician, every number. Quality is high because the person who cares most is watching everything. A practice in this state often produces better clinical work than a larger, more systematized competitor, and that early success is exactly what makes the ceiling so easy to hit. The founder concludes that personal oversight is the reason the practice is good, and so personal oversight becomes the thing the founder protects as the practice grows.
Growth then disguises the problem. A practice that opens a second location can spend six to twelve months in operational disruption that registers internally as the normal cost of growing rather than as a structural warning. The clinical fidelity that held when one BCBA leadership group could see every session becomes harder to hold when leadership is split across two sites and direct supervisory contact drops. The hiring quality that depended on the founder personally vetting each candidate becomes harder to maintain when hiring volume forces delegation. The practice that opens a second site often discovers that founder oversight was the operating system, and that it does not run on two machines at once.
What the ceiling actually is
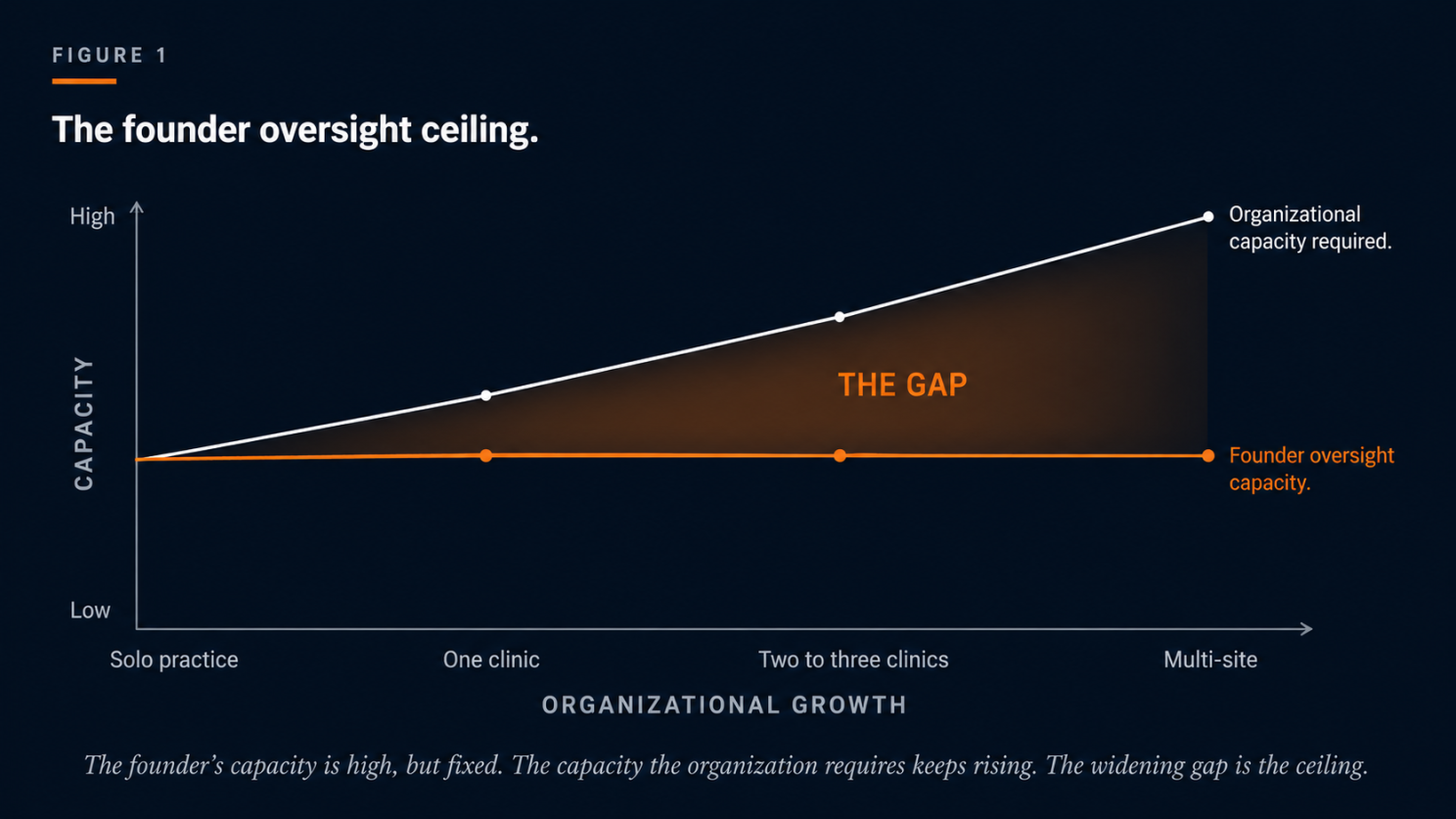
The clearest way to see the ceiling is to separate two things that start out looking identical and then diverge. One is the founder’s capacity to personally oversee the work. The other is the capacity the organization actually requires to oversee its work. In a solo practice, these are the same. The founder can see everything because there is little to see. As the practice grows, the capacity required to oversee clinical quality, operations, finance, hiring, compliance, and the development of other leaders rises with every stage of growth. The founder’s personal capacity does not rise with it. There are only so many hours, and only one person.
The gap between rising required capacity and fixed founder capacity is the founder oversight ceiling. It widens at every stage of growth, and it cannot be closed by working harder, because the constraint is not effort. The constraint is that one person’s attention does not scale.
This is not a leadership failure
The instinct, when a founder hits this ceiling, is to read it as a personal failing. The founder did not delegate enough, did not let go, did not trust the team. That was the reading I held about myself for too long, and it is wrong, and it is worth being precise about why, because the wrong diagnosis produces the wrong intervention.
The founder is not the cause of the gap. The absence of systems beneath the founder is the cause. When a practice has no accountability structure, no documented processes, no scorecards, and no developed leaders, founder oversight is not a choice the founder is making instead of delegating. It is the only mechanism that exists. You cannot delegate clinical quality oversight to a supervisor when no one has defined what that oversight consists of or trained anyone to do it. You cannot hand off hiring when the standard for a good hire lives only in the founder’s head. The founder is doing everything because everything was built to run through the founder, and usually no one built it that way on purpose. It happened by accretion, one absorbed responsibility at a time, while the founder was busy keeping the practice alive.
This matters because it tells you where to intervene. A character reading sends you toward founder coaching, delegation workshops, and time-management systems, and none of those close the gap, because the gap is not made of the founder’s habits. A structural reading sends you toward building the systems that let organizational standards reach the front line without traveling through the founder every time. That is the work that actually raises the ceiling.
Why performer-level fixes do not raise the ceiling
When a practice hits this ceiling, the symptoms show up at the level of individual people. A technician drifts from protocol. A new supervisor makes a call the founder would not have made. A clinician leaves. The natural response is to intervene at the level where the symptom appeared, which means more training, more feedback, a new hire to replace the one who left. These are performer-level interventions, and the behavioral science is clear that the field has leaned on them heavily. Gravina and colleagues (2018) reviewed organizational behavior management research in human service settings across more than two decades and found that the large majority of intervention studies targeted the individual performer, with interventions at the process and organization levels appearing rarely.
Performer-level work is necessary, and it is not sufficient, because the founder oversight ceiling does not originate at the performer level. It originates at the organization level, in the absence of structure, and a problem that originates above the performer cannot be resolved by intervention at the performer. Training a technician does not build the supervision system that would have caught the drift earlier. Replacing a clinician who left does not address the conditions that made the role unsustainable. The same problem returns in the next person, because the conditions that produced it are still in place. The work that raises the ceiling happens at the level where the ceiling lives.
What raises the ceiling
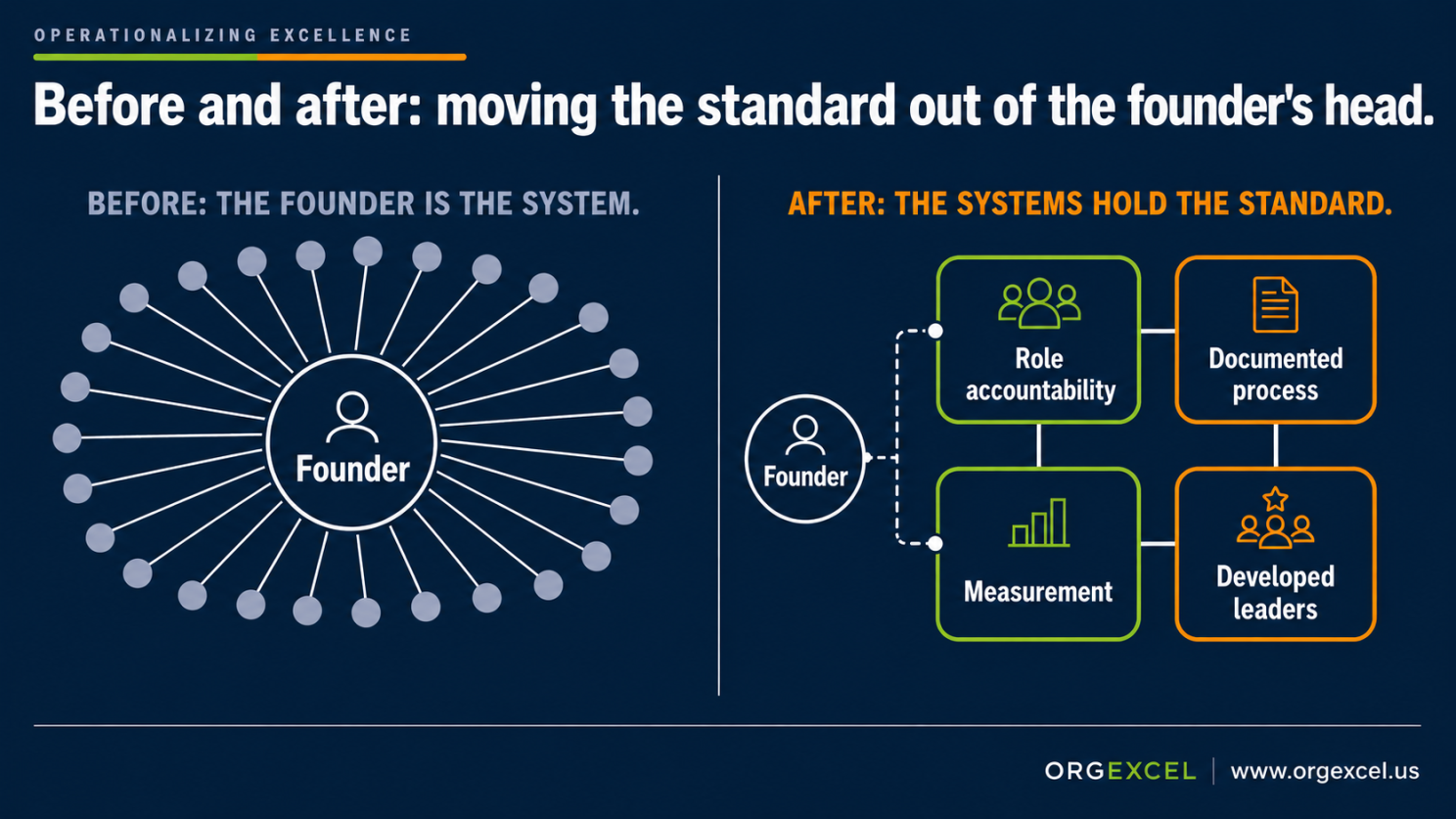
Raising the ceiling means building the systems that let organizational standards reach the front line without the founder personally carrying them there. The behavioral science gives a reasonably clear order of operations, and the order matters as much as the systems themselves.
The first system is role accountability. Before anything can be delegated, the organization has to define who owns what, to what standard, measured how. This is not an org chart, which shows reporting lines. It is a structure that names accountabilities and the results each one is responsible for producing. Novak et al. (2019) describe evidence-based performance management as resting first on clearly defined expectations and the initial training that makes those expectations achievable, before any ongoing feedback can do its work. You cannot manage performance against a standard that was never made explicit, and you cannot hand a responsibility to someone who was never told what the responsibility actually entails. The accountability structure is what makes delegation possible, because it converts the standard that lived in the founder’s head into a standard the organization can see.
The second system is documented process. Most of what a founder does to hold a practice together is procedural knowledge that has never been written down. How intake actually flows. How a case gets staffed. What happens when a technician calls out. Luke et al. (2024) describe process mapping as a practical method for making this implicit organizational knowledge explicit, walking practitioners through the steps of capturing how work actually moves so that it can be examined and improved. A process that exists only in the founder’s practice cannot be taught, cannot be measured, and cannot be improved by anyone other than the founder. Writing it down is what lets someone else run it.
The third system is measurement that reaches every level. Once accountabilities are defined and processes are documented, the organization needs to know whether the standard is being met without the founder having to personally check. This is the role of scorecards and the regular review of them. Locke and Latham (2002), summarizing decades of research, established that specific, measurable goals reviewed on a cadence account for a substantial share of the difference in performance between individuals and groups. The scorecard is the mechanism that lets a supervisor, rather than the founder, see whether the work is on standard, and the cadence of review is what keeps the standard alive rather than posted and forgotten.
The fourth system is developed leaders, and it is the one that finally raises the ceiling, because it is the one that creates more people capable of holding the standard. The first three systems make the standard explicit, documented, and measurable. The fourth puts trained people in position to own it. This is where the connection between daily work and the organization’s larger purpose has to be made deliberately rather than left to chance. Carton (2018), in a detailed study of how NASA leadership built a sense of shared mission, found that people did their best work when leaders drew an explicit line between an individual’s concrete daily tasks and the organization’s larger objective, rather than assuming that line was obvious. In a practice, this is the difference between a supervisor who runs sessions and a supervisor who understands how their clinic’s performance connects to what the organization is trying to be. Developing that understanding in other people is what lets the founder stop being the only person who holds the whole picture.

A worked example
A practice owner notices that fidelity has slipped at the second location. Two technicians are running programs with measurable drift, and a third just gave notice. The owner’s first instinct is to schedule a training for the two who are drifting and to start recruiting to backfill the one who is leaving. That is the performer-level read, and it will produce a short improvement followed by the same problem in the next set of technicians.
The structural read starts one level up. The second location has no on-site BCBA with defined supervisory accountabilities, because when the location opened, supervision was something the founder did on visits. The supervision cadence that held at the first location was never a system. It was the founder being present. At the second location, the founder cannot be present often enough, so the standard erodes for every technician at that site, including the ones whose drift has not surfaced yet. The technician who gave notice is not leaving because of a personal failing. The conditions, an unsupervised site with no clear ownership of clinical quality, are the same conditions Plantiveau et al. (2018) and Novack and Dixon (2019) identify as the structural predictors of burnout and turnover in this workforce, and Nastasi et al.(2024) heard described directly when registered behavior technicians named inconsistent supervision and unclear support as reasons they left.
The intervention that raises the ceiling is not the training, though training may still help once the structure is in place. The intervention is to define a supervisory accountability for the second location, place a developed leader in it, give that role a documented supervision process and a scorecard the founder can review without being on-site, and review it on a set cadence. That work takes the clinical-quality standard out of the founder’s physical presence and builds it into a system that operates at the second location whether the founder is there or not. The training sits downstream of that structural work, and it holds because the structure holds it.
What this changes for the practice owner
The practical shift is in what you do first when you hit the wall. The founder who reads the ceiling as a personal failing works harder, delegates anxiously, and burns out, because effort is not the constraint. The founder who reads it as a structural condition does something different. They stop trying to personally scale their own attention and start building the systems that let the organization’s standards travel without them.
That is a hard shift, because the systems take time to build and the founder’s personal oversight produces results today. Building the accountability structure, documenting the processes, standing up the scorecards, and developing the leaders is slower than just handling it yourself, and for a while it feels less efficient. The discipline this requires is the willingness to build the system before the growth event forces it, rather than after the growth event has already exposed that the system was missing. A practice that scales before the infrastructure exists becomes a practice in crisis within a year to eighteen months. A practice that builds the infrastructure first earns the scale.
The encouraging part of the structural reading is that it runs on the same logic you already use in clinical work every day. You would not write an intervention before you understand what maintains the behavior. You assess first, identify the controlling variables, and only then design a plan that addresses them. The founder oversight ceiling can be read the same way. The behavior worth analyzing is the founder's own, the constant stepping in to check, correct, and hold the line, and that behavior is doing real work, so it persists. Each time the founder steps in, the problem resolves and the standard is met, which reinforces stepping in again next time. The four systems are what would otherwise hold the standard in place, and while they are missing, the only thing that reliably produces the result is the founder's presence. Build the systems and you change the contingency, so that meeting the standard no longer depends on the founder being the one to act. You already have the analytic skill this calls for. The shift is in pointing the assessment-before-intervention discipline you apply to a client upward, toward the organization that surrounds that client.
What is next in the series
This article applied the diagnostic frame from Article 01 to the single structural condition that limits most growing ABA practices. The systems that raise the ceiling, the accountability structure, the documented processes, the scorecards, and the leadership pipeline, each develop along a defined path as an organization matures, and each becomes the subject of its own article in this series. The next piece takes on the first of them, the accountability structure, and what it actually takes to move a standard out of the founder’s head and into a form the organization can hold.
References
Carton, A. M. (2018). “I’m not mopping the floors, I’m putting a man on the moon”: How NASA leaders enhanced the meaningfulness of work by changing the meaning of work. Administrative Science Quarterly, 63(2), 323–369. https://doi.org/10.1177/0001839217713748
Gravina, N., Villacorta, J., Albert, K., Clark, R., Curry, S., & Wilder, D. (2018). A literature review of organizational behavior management interventions in human service settings from 1990 to 2016. Journal of Organizational Behavior Management, 38(2–3), 191–224. https://doi.org/10.1080/01608061.2018.1454872
Locke, E. A., & Latham, G. P. (2002). Building a practically useful theory of goal setting and task motivation: A 35-year odyssey. American Psychologist, 57(9), 705–717. https://doi.org/10.1037/0003-066X.57.9.705
Luke, M. M., Dams, P., & Lichtenberger, S. N. (2024). Improving human-service organizations through process mapping: A tutorial for practitioners. Behavior Analysis in Practice, 17(1), 359–370. https://doi.org/10.1007/s40617-024-00906-4
Nastasi, J. A., McGarry, K. M., Peters, K. P., Leon, Y., Bacotti, J. K., & Gravina, N. (2024). A qualitative analysis of variables contributing to Registered Behavior Technicians’ burnout and turnover in Florida. Behavior Analysis in Practice, 18(4), 1139–1151. https://doi.org/10.1007/s40617-024-01033-w
Novack, M. N., & Dixon, D. R. (2019). Predictors of burnout, job satisfaction, and turnover in behavior technicians working with individuals with autism spectrum disorder. Review Journal of Autism and Developmental Disorders, 6(4), 413–421. https://doi.org/10.1007/s40489-019-00171-0
Novak, M. D., DiGennaro Reed, F. D., Erath, T. G., Blackman, A. L., Ruby, S. A., & Pellegrino, A. J. (2019). Evidence-based performance management: Applying behavioral science to support practitioners. Perspectives on Behavior Science, 42(4), 955–972. https://doi.org/10.1007/s40614-019-00232-z
Plantiveau, C., Dounavi, K., & Virués-Ortega, J. (2018). High levels of burnout among early-career board-certified behavior analysts with low collegial support in the work environment. European Journal of Behavior Analysis, 19(2), 195–207. https://doi.org/10.1080/15021149.2018.1438339
