The chart that effectively runs your ABA practice
Operationalizing Excellence | Article 03 in a series drawn from Building Organizational Excellence: A Behavioral Systems Approach for ABA Practice Owners.
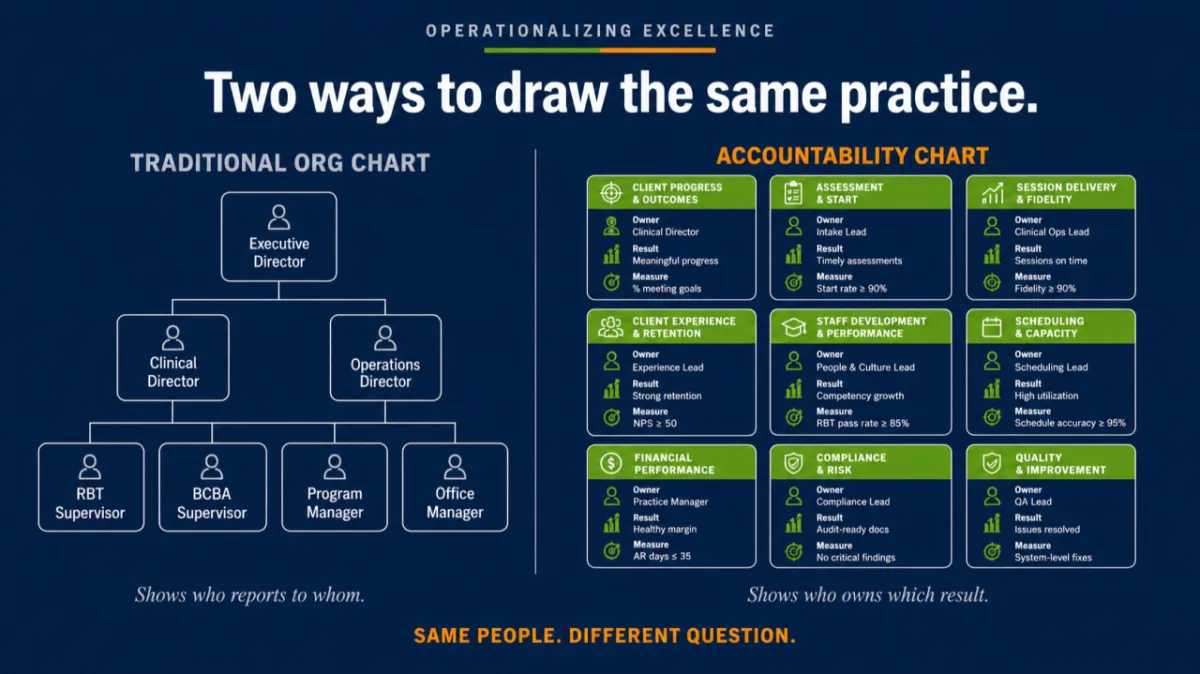
The org chart that does not actually run anything
Most ABA practices have an org chart. It shows who reports to whom, with the founder at the top, the clinical director and the operations lead below, and the supervisors and technicians filling out the lower rows. It is a useful picture of reporting lines, and it is almost useless for running an organization, because it answers a question that rarely causes the problem. The question an org chart answers is who reports to whom. The question that actually determines whether work gets done is who owns what result, and the org chart does not answer that.
The previous article in this series described the founder oversight ceiling, the structural condition where the founder is the only mechanism delivering organizational standards to the front line, and named the four systems that raise it. The first of those systems is the accountability structure, and it comes first for a reason. You cannot delegate a responsibility, you cannot measure it, and you cannot develop someone to own it until the responsibility itself has been defined as a specific result that one named person is accountable for producing. The accountability structure is the work of making that definition, and it is the foundation the other three systems are built on.
What an accountability structure actually is
An accountability structure names the results an organization must produce, assigns each result to one owner, and defines each result in terms specific enough that two people would agree on whether it was met. That last part is the difference between an accountability structure and a list of job titles. A title names a role. An accountability names a result and the person responsible for it, stated so clearly that its status is observable.
This is the same discipline a behavior analyst already applies to clinical work, moved up to the level of the organization. In clinical practice, a vague target like improving communication is useless until it is pinpointed into an observable, measurable behavior that two observers would score the same way. Wilder and Cymbal (2023) describe pinpointing as the first methodological step in organizational behavior management, defining a behavior or result with enough precision that independent observers would agree on whether it occurred. An accountability structure applies pinpointing to organizational results. Owning clinical quality is not an accountability, because two people would not agree on whether it was being met. Maintaining treatment-plan fidelity at or above ninety percent across all active cases, measured monthly, is an accountability, because its status is observable and the result belongs to a named person. Treatment-plan fidelity here means the percentage of the written plan’s steps that are implemented as written, scored through direct observation of a sample of sessions. The number matters less than the fact that it is defined, observable, and owned.
Why the distinction from the org chart matters
The org chart and the accountability structure answer different questions, and confusing them is one of the most common reasons delegation fails in a growing practice. When a founder says they have delegated clinical quality to the clinical director, they usually mean the clinical director sits above the supervisors on the org chart. They rarely mean that the clinical director owns a pinpointed clinical-quality result, knows what that result is, and is measured against it. The reporting line moved, but the accountability did not, because the accountability was never defined as a result in the first place. It lived in the founder’s head as a standard the founder personally enforced, and a reporting line cannot carry a standard that was never written down.
This is why simply hiring senior people does not raise the founder oversight ceiling. Novak and colleagues (2019) describe evidence-based performance management as resting first on clearly defined expectations and the initial training that makes those expectations achievable, before any feedback or consequence can do its work. A new clinical director placed above the supervisors on the org chart, but handed no pinpointed result and no definition of what owning clinical quality means in this practice, is in the same position the founder was, holding a standard that exists only as personal judgment. The accountability structure is what converts that personal judgment into an organizational result the new leader can actually own.
Building one: the four questions for each seat
An accountability structure is built one seat at a time, and each seat is defined by answering four questions. The questions are simple, and the discipline is in answering them precisely rather than approximately.
See content credentials

The first question is what result this seat is accountable for producing. The unit here is the outcome the organization is counting on from this seat, rather than the list of tasks the person performs. The shift from tasks to results is the hard part, because most roles are described as lists of activities. A scheduling seat is not accountable for managing the schedule, it is accountable for a result such as billable-hour utilization staying at or above a target percentage of authorized hours.
The second question is who owns it. One name, not a committee and not a department. An accountability owned by everyone is owned by no one. Diener and colleagues (2009) describe behavioral systems analysis as the work of identifying where organizational processes connect and disconnect, and a result with no single owner is a guaranteed disconnect, because when performance drops there is no one whose job it was to prevent it.
The third question is how the result is measured. This is the pinpointing step. A result that cannot be observed and measured is not an accountability, it is an aspiration. The measure does not have to be elaborate, but it has to be specific enough that the owner and the founder would agree on whether the result was met this month.
The fourth question is how often it is reviewed. An accountability with no review cadence decays into a title, because nothing in the system checks whether the result is still being produced. Locke and Latham (2002), summarizing decades of goal-setting research, established that specific goals reviewed on a regular cadence account for a substantial portion of the difference in performance between individuals and groups. The cadence is what keeps the accountability alive.
Where founders get stuck
The most common place a founder stalls is the third question, the measurement, because it forces a precision the founder has been carrying informally. It is easy to say the clinical director owns clinical quality. It is hard to say exactly what observable result defines clinical quality in this practice, because the founder has been judging it by feel for years. That difficulty is not a sign the exercise is going wrong. It is the exercise. The reason clinical quality could not be delegated was that it had never been pinpointed, and pinpointing it is precisely the work that makes delegation possible.
The second common place founders stall is wanting to assign a result to more than one person because the work genuinely crosses roles. Authorization management touches intake, clinical, and billing, and the temptation is to make all three accountable. The discipline is to name one owner for the result, the person accountable for the authorized hours being captured and used, while the others contribute to the process. Shared work is normal. Shared accountability is how results fall through the gap between people, each assuming another owned it.
One more thing to expect, especially early. The seats in an accountability structure are results, not headcount, so a small practice will have one person holding several seats at once. The founder may own clinical quality, operations, and payroll all at the same time. That is normal and it is not the problem. The structure still names each result separately, records who currently holds it, and sets the condition that will trigger hiring a dedicated owner, for example when the practice passes a certain client count or opens a second site. Built this way, the accountability structure doubles as a hiring plan, because it shows exactly which results the founder is carrying and the point at which each one should move to someone else. The build tool and workbook that go with this article record the current owner and the hiring trigger for every seat.
A Worked Example Exists and You Can Start From It
Reading about an accountability structure is not the same as building one, and the fastest way to build one well is to study a complete example before starting your own. The resources that go with this article include a fully built accountability structure for a fictional mid-size ABA practice, with every seat named, every result pinpointed, and the reasoning behind each one explained, alongside an interactive tool you can use to build and print your own. The example is there because the pinpointing skill is learned by seeing it done, and the build tool is there because the structure is a living document you will return to as the practice grows. Both are free inside the Operationalizing Excellence community, along with every other resource in this series.
COMPANION RESOURCES. Three tools go with this article, all free inside the Operationalizing Excellence community. An interactive accountability-structure builder that walks you through a worked example and then lets you build, save, and print your own. A read-only guide that explains the worked example seat by seat, including why each result is pinpointed the way it is. And an Excel workbook with the master accountability map and a scorecard tab for every role, including the BCBA and RBT performer roles, each recording its priority accountability, its current owner, and the trigger for hiring a dedicated owner as the practice grows. Join the community to get all three, and everything else released in this seriesThe practical move this article asks for is not large, and it is not fast. It is to take the standards you currently carry in your head, one at a time, and write each one as a result that a named person owns and that can be measured. That is the accountability structure. It is the first of the four systems that raise the founder oversight ceiling, and it is the one the others depend on, because a process you document, a scorecard you build, and a leader you develop all require that the result they are organized around has first been defined.
What is next in the series
This article built the first of the four systems that raise the founder oversight ceiling. The next takes on the second, documented process, and the work of capturing how the practice actually operates so that the work can be taught, measured, and improved by someone other than the person who has always done it.
References
Diener, L. H., McGee, H. M., & Miguel, C. F. (2009). An integrated approach for conducting a behavioral systems analysis. Journal of Organizational Behavior Management, 29(2), 108–135. https://doi.org/10.1080/01608060902874534
Locke, E. A., & Latham, G. P. (2002). Building a practically useful theory of goal setting and task motivation: A 35-year odyssey. American Psychologist, 57(9), 705–717. https://doi.org/10.1037/0003-066X.57.9.705
Novak, M. D., DiGennaro Reed, F. D., Erath, T. G., Blackman, A. L., Ruby, S. A., & Pellegrino, A. J. (2019). Evidence-based performance management: Applying behavioral science to support practitioners. Perspectives on Behavior Science, 42(4), 955–972. https://doi.org/10.1007/s40614-019-00232-z
Wilder, D., & Cymbal, D. (2023). Pinpointing, measurement, procedural integrity, and maintenance in organizational behavior management. Journal of Organizational Behavior Management, 43(3), 221–245. https://doi.org/10.1080/01608061.2022.2108537
